Cardiovascular diseases are the number one cause of death globally, taking an estimated 17.9 million lives each year, 52.5% of which are attributed to coronary heart disease. Consequently, related symptoms are taken very seriously: In patients with suspected coronary heart disease, the presence of a stenosis - an abnormal narrowing in a blood vessel, has to be verified, its extent assessed, and the need for revascularisation determined.
Gold standard: catheter-based FFR and non-hyperaemic pressure ratios
In patients with coronary artery disease, it’s critical that the hemodynamic relevance of a stenosis is assessed correctly. Catheter-based Fractional Flow Reserve (FFR) assessment is considered the gold standard by international guidelines. The hemodynamic recording system Sensis Vibe smoothly integrates FFR measurement for an optimal workflow.

Benefits: Vendor-independent FFR measurement with Sensis Vibe; Can also display non-hyperaemic indices, e.g. dPR
Less invasive: angio-derived FFR
 Pressure wires and hyperaemic stimuli can cause patient discomfort, are cost- and time-consuming – and they can’t be used in all patients with a coronary stenosis.
Pressure wires and hyperaemic stimuli can cause patient discomfort, are cost- and time-consuming – and they can’t be used in all patients with a coronary stenosis.
Angio-derived FFR is a less invasive option: A software algorithm calculates the Fractional Flow Reserve (FFR) value based on images delivered by the angio systems.
This means shorter, less stressful examinations and less dose for you and your patients.
Benefits:
No additional interventional risks for patients; Fast workflow and less material needed; Patient is already on the table if a stent needs to be placed.
Non-invasive: CT-based FFR
 Can diagnostics be eased for patients with a suspected coronary stenosis but no acute symptoms?
Can diagnostics be eased for patients with a suspected coronary stenosis but no acute symptoms?
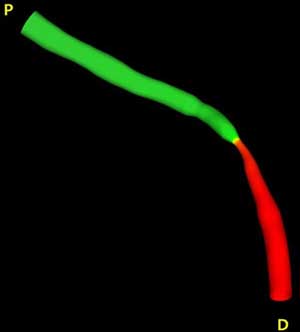
A gentle alternative to the gold standard for Fractional Flow Reserve (FFR) assessment is CT-FFR: Using high-quality images from the Dual Source CT scanners, a software creates an arterial 3D model to simulate the blood flow – so you can determine the presence and functional significance of a coronary stenosis without an invasive procedure.
Benefits:
No interventional risks for patients; Fewer unnecessary invasive procedures; Opportunity to reduce overall costs to healthcare system by 26%
Description of the technology
HeartFlow FFRCT is coronary physiology simulation software used for the qualitative and quantitative analysis of previously acquired computerised tomography DICOM data (Digital Imaging and Communications in Medicine). The software provides a non-invasive method of estimating fractional flow reserve (FFR) using standard coronary CT angiography (CCTA) image data. FFR is the ratio between the maximum blood flow in a narrowed artery and the maximum blood flow in a normal artery. FFR is currently measured invasively using a pressure wire placed across a narrowed artery.
After a clinician decides to request a HeartFlow test, anonymised data from a CCTA scan (of at least 64 slices) are sent from the local imaging system, by secure data transfer to HeartFlow's central processing centre in the US. A case analyst employed by the company then uses the image data to create 3D computer models of the coronary arteries, incorporating coronary flow characteristics. The results are presented in a report which is sent, by secure data transfer, to the referring clinician within 48 hours. The report includes both 3D images of the coronary anatomy and calculated functional information, including the estimated FFR values (known as FFRCT values). Clinicians can then use the report to help guide the management of suspected coronary artery disease.
HeartFlow FFRCT is intended for use in patients with stable, recent onset chest pain and suspected angina. Because the safety and effectiveness of FFRCT analysis has not been evaluated in other patient subgroups, HeartFlow FFRCT is not recommended in patients who have an acute coronary syndrome or have had a coronary stent, coronary bypass surgery or myocardial infarction in the past month.
The claimed benefits of HeartFlow FFRCT were as follows:
- Analysis is done using standard CCTA scans, without the need for additional imaging, radiation or medication.
- It provides the same accuracy in excluding coronary artery disease as CCTA, and characterises the coronary arteries from both functional and anatomical perspectives, differentiating between ischaemic and non-ischaemic vessels in a way that CCTA cannot.
- It allows physicians to evaluate anatomic coronary artery disease and accurately determine which coronary lesions are responsible for myocardial ischaemia, avoiding unnecessary invasive diagnostic or therapeutic procedures and related complications.
- It reduces the need for revascularisation in patients after identifying anatomic stenosis by invasive coronary angiography (ICA) alone, by more accurately identifying if those stenoses are ischaemic.
- It improves the diagnostic accuracy for coronary artery disease compared with CCTA alone against the gold standard of invasive FFR, and provides both functional and anatomic assessment of coronary arteries.
- It has better diagnostic performance than CCTA alone, or other non-invasive or invasive tests (such as nuclear myocardial perfusion, magnetic resonance perfusion, stress echocardiography, exercise treadmill testing, invasive angiography or intravascular ultrasound) for detecting and excluding coronary artery lesions that cause ischaemia.
- It reduces costs arising from inconclusive or inaccurate diagnostic tests.
- It avoids staff and procedure costs for unnecessary ICAs.
- It avoids staff and procedure costs for unnecessary interventions (such as angioplasty).
In conclusion, non-invasive CT for Fractional Flow Reserve (FFR) provides a more effective use of high-cost invasive procedure suites, providing the opportunity to reduce waiting times for these facilities and increase patient turnaround.
Sources:
https://www.nice.org.uk/guidance/mtg32
https://www.siemens-healthineers.com/angio/innovations-technologies/ffr
https://www.heartflow.com/heartflow-ffrct-analysis/
https://en.wikipedia.org/wiki/Stenosis