Why should healthcare organisation buy new healthcare technology?
Why should healthcare organisation buy new healthcare technology?
This sounds like an obvious question, but it is a highly complex. Healthcare technology means different things to different people.
The document ‘Delivering the Forward View: NHS planning guidance: 2016/17 – 2020/21’ https://www.england.nhs.uk/wp-content/uploads/2015/12/planning-guid-16-17-20-21.pdf hardly mentions medical equipment except to say:
36. Capital investments proposed by providers should be consistent with their clinical strategy and clearly demonstrate the delivery of safe, productive services with a business case that describes affordability and value for money. Given the constrained level of capital resource available from 2016/17, there will be very limited levels of financing available and the repayment of existing and new borrowing related to capital investment will need to be funded from within the trust’s own internally generated capital resource in all but the most exceptionally pre-agreed cases. Trusts will need to procure capital assets more efficiently, consider alternative methods of securing assets such as managed equipment services, maximize disposals and extend asset lives.
There are many stakeholders with different views, and in many cases, opposing views on how medical technology should be procured. We would all like to think that patients have access to the best technology to enable the best delivery of care.
I know from my own experience that whether we are working in the public sector or the private sector, many healthcare organisations are working with equipment and software that is often outdated. In some organisations, especially the National Health Service, there is very little or no planned replacement program, and little or no capital funds.
The finger for not replacing healthcare technology is often pointed at a lack of funding, and this is sometimes true. The government need to decide how much money to put into the system, and the healthcare managers then need to decide how best to spend that money. Often, the issue can be not having the expertise within the organisation to do the equipment planning and replacement strategies.
To decide which types of technology to replace, and when to replace, requires a complex set of data and an understanding of the activities of the organisation. Some organisations have a senior management team that meets regularly to review business cases and to decide what to buy, and went to buy it. This management team normally consists of a broad range of stakeholders that may include: finance, procurement, clinicians, nurses, IT managers, Estates managers, Clinical depts. managers, etc. It needs this multiple stake holder approach because it is such a technically and clinically complex process.
The impact of buying new technology will have an impact on the overall budget of the organisation, which means an increase in cost for the purchase of the technology, but correspondingly, it has an impact on improving patient care and outcomes. If the impact on the patient is positive, and means the patient will leave the hospital sooner, get well quicker, or not need any follow-up treatment, then the increased impact on the technology budget is outweighed by the impact on the patient in terms of both clinical outcomes, and cost.
The average acute hospital will spend less than 4% of its overall budget on technology, but it impacts all areas. When setting budgets for technology replacement planning, it must not be overlooked that the technology not only improves clinical outcomes, but when implemented correctly, can also delivers substantial productivity improvements leading to cost savings (or increased revenues) that offset the original investment.
As an illustrative example of how technology can improve clinical outcomes, and also improve productivity, we can look to the latest 3-D cone beam CT imaging technology.
These new types of technology are expensive, but deliver more accurate models for surgical implants or reconstruction, at much higher accuracy than a consultant creating a 3-D model mathematically from a 2-D radiographic image.
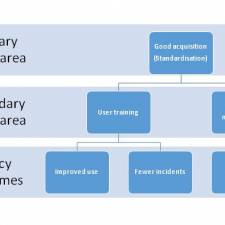
Firstly,
- specifying the asset needed, and explaining the time it takes for a consultant surgeon to create a model from a 2-D image may be as much as 30 minutes (Approx. £35 in pay), but in comparison, the time it takes to do this using the latest 3-D technology is less than 15 seconds, allowing for more patients to be seen. 1 extra patient per day covers the investment in the asset, 2 extra, means the Trust is earning more income. The business case allows for:
- funding of the asset to be agreed. Once the asset funding was agreed, it was
- bought and added to the database, followed by installation and
- user training. This allows the consultant to see many more patients, and also have more confidence in the clinical outcomes. Training for engineers could also be added into the process, or alternatively, take out a
- maintenance contract with the supplier. This process should be part of the organisations business
- plan for additions and deletions. This process can only succeed through
- communication with all stakeholders involved. (In this case, Diagnostic imaging manager, Maxillo facial consultants, IT manager, procurement manager, estates manager, EBME manager, radiation protection advisors, healthcare technology improvements board) This is just one of many illustrations of how technology can improve productivity and deliver better clinical outcomes.

In most organisations, they do not have the time or money to develop or implement technology plans. This creates a lag in service improvement as modern technology is not adopted when it becomes available. That ‘time lag’ from when it is available to being in use may have a number of factors contributing to the slow take up.
For example, the clinical consultants do not normally have the time, and do not understand the complex forms, process, and approval routes to complete business cases; they therefore rely on their management teams to do that on their behalf. Often, the management teams do not properly understand what the decision-makers (such as finance directors, Estates directors, CEO’s, medical directors, nursing directors, IT directors, etc.) are looking for and therefore the new technology does not get approved or implemented.
It is imperative that the policies within the organisation reflect on the financial, clinical, and operational aspects of the organisation with regard to technology planning. If the organisation brings together the right people, it can deliver all aspects of healthcare technology management.
Every organisation should allocate a healthcare technology management team to address the practical issues involved with specifying, procuring, and implementing new technology. There should be goals and plans that are set out by the healthcare technology management team, and followed up on a regular basis to ensure those goals and plans are on track. To enable this to happen means that the financial officers for the organisation must allocate sufficient funds for all healthcare technology management activities, which can include: Specifications; business case production; procurement; user training; maintenance, and governance.
How can senior healthcare managers deliver financially sustainable models for healthcare technology replacement planning?
The healthcare technology management policy should be the starting point that outlines and guides the practices needed within the organisation to deliver sustainable models for replacement planning. This does not mean an inflexible and rigid of management - financial control is required.
Each group of technology needs to be considered by its users, and by the healthcare technology management team, with a view on how long that technology will remain current, and to create timelines for replacement for each type of technology used across the organisation.
On average, an acute organisation may use 400 to 500 different types of technology. Even if these are phased over a 7 to 10 year cycle, it requires a major planning and procurement exercise to enable the technology to be replaced on time, and to ensure it is the right time.
Sometimes, even though there is a plan to replace a group of technology, it may not be appropriate because there has been little or no technological change, and therefore the life of the devices can be extended. It is difficult to predict this when you buy the devices, so normally an indicative lifetime would be given to each technology group, with a degree of flexibility.
More information on healthcare technology management strategies can be found in the management section of the EBME website:
Further reading:
Healthcare Technology Innovation and Policy.
Healthcare Technology Procurement Policy
Technology as an enabler to improve NHS productivity and reduce costs.
The impact of device acquisition on device management.
The Sandham Model - Action Research for Healthcare Managers
Managed Facility Contracts in the NHS - Trends and Benefits
Dr. John Sandham