by Smith, E.J.
Introduction
The electroencephalogram (EEG) is a recording of the electrical activity of the brain from the scalp. The first recordings were made by Hans Berger in 1929 although similar studies had been carried out in animals as early as 1870.
The waveforms recorded are thought to reflect the activity of the surface of the brain, the cortex. This activity is influenced by the electrical activity from the brain structures underneath the cortex.
 EEG traces
EEG traces
The nerve cells in the brain produce signals that are called action potentials. These action potentials move from one cell to another across a gap called the synapse. Special chemicals called neurotransmitters help the signals to move across the gap. There are two types of neurotransmitters, one will help the action potential to move to the next cell, the other will stop it moving to another nerve cell.
The brain normally works hard to keep an equal amount of each of these neurotransmitters in the brain.
EEG activity is quite small, measured in microvolts (µV) with the main frequencies of interest up to approximately 30 Hertz (Hz).
Electrodes
Small metal discs called electrodes are placed on the scalp in special positions. These positions are identified by the recordist who measures the head using the International 10/20 System. This relies on taking measurements between certain fixed points on the head. The electrodes are then placed at points that are 10% and 20% of these distances.
Each electrode site is labelled with a letter and a number. The letter refers to the area of brain underlying the electrode

10/20 System of electrode placement
- F - Frontal lobe
- T - Temporal lobe
- C - Central lobe
- P - Parietal lobe
- O - Occipital lobe
- Even numbers denote the right side of the head
- Odd numbers denaote the left side of the head.
There are a great variety of electrodes that can be used. The majority are small discs of stainless steel, tin, gold or silver covered with a silver chloride coating. These normally have a lead attached. Alternative methods consist of a cap in which the electrodes are already imbedded.
Montages
EEG machines use a differential amplifier to produce each channel or trace of activity. Each amplifier has two inputs. An electrode is connected to each of the inputs.
 Differential amplifier
Differential amplifier
Differential amplifiers measure the voltage difference between the two signals at each of its inputs. The resulting signal is amplified and then displayed as a channel of EEG activity.

Amplifier principles
The manner in which pairs of electrodes are connected to each amplifier of the EEG machine is called a montage. Each montage will use one of three standard recording derivations, common reference, average reference or bipolar.
Common reference derivation
Each amplifier records the difference between a scalp electrode and a reference electrode. The same reference electrode is used for all channels. Electrodes frequently used as the reference electrode are A1, A2, the ear electrodes, or A1 and A2 linked together.

Common reference derivation
Average reference derivation
Activity from all the electrodes are measured, summed together and averaged before being passed through a high value resistor. The resulting signal is then used as a reference electrode and connected to input 2 of each amplifier and is essentially inactive. All EEG systems will allow the user to choose which electrodes are to be included in this calculation.

Average reference derivation
Bipolar derivation
These sequentially link electrodes together usually in straight lines from the front to the back of the head or transversely across the head. For example the first amplifier may have electrodes FP1 and F3 connected to it and the second amplifier F3 and C3 connected to it.

Bipolar derivation
Analogue EEG instruments
Conventional analogue instruments consist of an amplifier, a galvanometer and a writing device. A galvanometer is a coil of wire inside a magnetic field. The output signal from the amplifier passes through the wire causing the coil to oscillate. A pen mounted on the galvanometer moves up and down each time the coil moves. The pen draws the trace onto paper moving below it.
The amplifier output is controlled by high and low frequency filters and sensitivity controls. The high and low frequency filter values will set the window within which the EEG activity is recorded. This is known as the bandwidth. The sensitivity controls the size of the activity displayed. For example a sensitivity of 10 µV/mm means that a signal with an amplitude of 100 µ V will produce a 1 cm vertical deflection.
The speed at which the paper moves on will also affect the appearance of the waveforms.
Digital EEG instruments
A digital EEG system converts the waveform into a series of numerical values. This process is known as Analogue-to-Digital conversion (ADC).
 Analogue waveform
Analogue waveform
The values can be stored in the computer memory, manipulated and then redisplayed as waveforms on a computer screen. The rate at which the waveform data is sampled in order to convert it into a numerical format is known as the sampling rate.
The sampling rate is usually expressed in Hz, for example 240 Hz is 240 times per second. The minimum acceptable sampling rate is 2.5 times greater than the highest frequency of interest but most digital EEG systems will sample at 240 Hz.
 Sampling rate of 240 Hz
Sampling rate of 240 Hz
Some recordings which involve recording activity directly from the brain surface, may have activity of a higher frequency, for example 200 Hz. Therefore some digital EEG systems will have optional sampling rates of 480 Hz available.
Sampling at rates lower than this will mean that when the signal is converted back to analogue form, it will not resemble the original waveform.
 Sampling rate of 50 Hz
Sampling rate of 50 Hz
A second factor that affects the accuracy of the waveform is sampling skew. Sampling skew occurs when all channels are not sampled simultaneously. Many digital EEG systems sample channel 1 first, then sample channel 2, then channel 3 etc. The time lag between sampling of each channel is known as sampling skew. To reduce the sampling skew, some digital systems use burst mode sampling. This increases the speed between successive channels sampling in order to reduce the amount of sampling skew.
A third factor that affects the accuracy of digital EEG waveforms is the display. The accuracy of a monitor display depends on the number of points or pixels that are available. The number of pixels available is referred to as the screen resolution. Screen resolution is described in numbers that represent the pixels available in the horizontal and vertical axis.
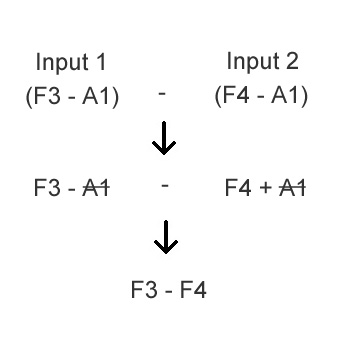
EEG signals that have been digitised can be manipulated to change the montage 'on-line' at the time of recording or 'off-line' after the recording is completed. This 'remontaging' is accomplished by recording all EEG channels with a common reference electrode. Regardless of the montage used to display the data while it is being recorded, data is stored into the computer memory in common reference mode. This allows the data to be displayed using different montages at a later time. Since digital systems store the analogue signal as numerical values, remontaging is a simple subtraction process which results in cancellation of the common reference.
An example is shown in the next figure.
The reference electrode A1 is common to both channels on input 2. It has the identical value in each channel. Remontaging these two channels together into one new channel is by subtraction which mathematically will cancel the value at the reference electrode. The resulting channel will therefore display the potential difference between F3 (input) 1 and F4 (input 2).
EEG Applications
One of the major roles of EEG is as an aid to diagnose epilepsy. Abnormal patterns such as spikes, sharp waves and/or spike and wave complexes can be seen. The type of activity and the area of the brain that it is recorded from will assist the physician in prescribing the correct medication for that type of epilepsy.
Patients with epilepsy that can not be controlled by medication will often have surgery in order to remove the damaged tissue. The EEG plays an important role in localising this tissue. Special electrodes can be inserted through the cortex or alternatively a grid of electrodes placed directly on the surface of the cortex. These recordings, often called Long Term Monitoring for Epilepsy (LTME), can be carried out for periods ranging from 24 hours to 1 week. The EEG recorded will indicate which areas of the brain should be surgically removed.
EEG studies can also be used in patients who are deeply unconscious, to distinguish between brain death and possible reversible conditions.
Electrocerebral inactivity (ECI) or electrocerebral silence (ECS) is defined as no EEG activity over 2 µ V in amplitude when recording from electrodes on the scalp, that are 10 cm or more apart.
Using the 10/20 International System of electrode placement, the average distance between electrodes in an adult is 6 to 6.5 cm. Activity recorded using these distances and at a normal display sensitivity may suggest ECS. However if the same activity was recorded using longer inter-electrode distances, some activity might be seen. Therefore some double distance electrode linkages are recommended for example FP1-C3, F3-P3, C3-O1 etc.
Display sensitivities of a minimum of 2 µ V/mm are required. However digital EEG systems have the added advantage of having sensitivity values of 1.5 and 1 µV/mm. This 50-100 % increase in sensitivity will allow a more confident assessment of the presence or absence of a 2 µV signal.
The EEG is also used to investigate other conditions that may affect brain function such as strokes, brain injuries, liver and kidney disease and dementia.
EEG Activity
EEG activity can be broken down into 4 distinct frequency bands:
- Beta activity > 13 Hz
- Alpha activity 8 Hz-13 Hz
- Theta activity 4 Hz-7 Hz
- Delta activity < 4 Hz
Beta activity is a normal activity present when the eyes are open or closed. It tends to be seen in the channels recorded from the centre or front of the head. Some drugs will increase the amount of beta activity in the EEG.

Beta activity
Alpha activity is also a normal activity when present in waking adults. It is mainly seen in the channels recorded from the back of the head. It is fairly symmetrical and has an amplitude of 40 µV to 100 µV. It is only seen when the eyes are closed and should disappear or reduce in amplitude when the eyes are open.

Alpha activity
Theta activity can be classed as both a normal and abnormal activity depending on the age and state of the patient. In adults it is normal if the patient is drowsy. However it can also indicate brain dysfunction if it is seen in a patient who is alert and awake. In younger patients, theta activity may be the main activity seen in channels recorded from the back and central areas of the head.

Theta activity
Delta activity is only normal in an adult patient if they are in a moderate to deep sleep. If it is seen at any other time it would indicate brain dysfunction.
Abnormal activity may be seen in all or some channels depending on the underlying brain problem.
Delta activity
There are a number of other waveforms which tend to be a little more specific to certain conditions.
For example spike and wave activity indicates a seizure disorder and may be seen in the EEG even if the patient is not having an epileptic seizure. Other epileptic conditions may be diagnosed if spikes or sharp waves are seen.

Spike and wave activity
Triphasic waves are sometimes seen if the patient has severe liver or kidney disease that is affecting brain function.
These are just brief descriptions of some of the simpler waveforms that may be seen in any one EEG recording. Combinations of any of the above patterns are possible which can make interpretation of the record difficult. Abnormal activity is not always specific to any condition and may suggest a few different diagnoses.
EEG Recording
The EEG recording can last from anything between 15 minutes to 1 hour or longer depending on the situation. Typically the patient will be lying down or sitting relaxed in a chair. Most of the recording is taken with the eyes closed, although the patient will be frequently asked to open them for short periods.
Most patients will be asked to carry out a period of deep breathing for approximately 3 minutes. This may produce some abnormal activity which would not be seen while the patient is relaxed. The physiological effect of deep breathing is to increase the amount of carbon dioxide (CO2) being removed from the bloodstream. This fall in CO2 produces a fall in blood pressure and at the same time blood vessels in the brain become constricted. This reduces blood flow and the delivery of oxygen and glucose to the brain. This in turn may produce some abnormal brain activity not seen in the resting record.
Photic stimulation is also carried out. A strobe lamp is placed 30 cm from the patient's eyes. Brief flashes of light (2 - 5 seconds in duration) at a number of different flash frequencies are delivered to the patient with both eyes open and eyes closed. A continuous flash with increasing and decreasing flash frequencies is sometimes used.
Some patients who are sensitive to flashing lights may show abnormal activity in the EEG.
Throughout the test the recordist is constantly annotating the record with any patient movements, or tasks that they are carrying out.
Other signals may also be recorded in conjunction with the EEG such as heart rate (ECG), respiration, eye movements (EOG), and muscle activity (EMG).
EEG Analysis
The EEG reports consists of a number of different sections. The recordist may prepare a report describing the type of activity seen in the record together with changes produced by deep breathing and photic stimulation. They will also comment on the patient's state during the recording. The physician will then interpret these changes with regard to the medical problem being investigated.
With an increase in the number of long recordings being carried out, many departments make use of detection algorithms such as spike and seizure detection. Although it is still necessary for the clinician to review the complete record, such programmes will mark and highlight sections of interest. The most efficient method of implementing these algorithms is for the detection to be carried out on-line.
Other methods of analysing EEG data include Power Spectrum Analysis. A Fast Fourier Transform (FFT) is performed on sections of EEG data to determine the power content of the four main frequency bands. The resulting waveforms can be displayed as a brain map which will show the scalp distribution of the power within each frequency band.
The amplitude of the different waveforms at a single point can also be displayed in a similar format.
This type of display provides a more objective analysis of the EEG activity compared to a subjective visual analysis by a physician.
Video monitoring
Simultaneous video monitoring of the patient during the EEG recording is becoming more popular. It allows the physician to closely correlate EEG waveforms with the patients activity and may help produce a more accurate diagnosis.
Domestic video recorders and cameras can be connected to an EEG machine using a time code generator. This records an accurate time signal onto the videotape. When the videotape and EEG are reviewed together the two signals are accurately synchronised together.
Video monitoring is always used for Long Term Monitoring recordings as the patient is unattended. The patient may also have an event button connected to the EEG machine so that times when the patient thought they were having an epileptic attack can be easily identified.
Sleep studies
The EEG is frequently used in the investigation of sleep disorders especially sleep apnoea. EEG activity together with other physiological signals such as heart rate, airflow, respiration, oxygen saturation and limb movement are measured simultaneously. These recordings are usually carried out overnight although some sleep studies can be carried out in the department during the day under strictly controlled conditions.
The EEG record can be broken down into epochs which are normally of 30 seconds duration. Using the EEG activity, each epoch is classified into one of 5 sleep stages. This is displayed visually as a Sleep Histogram.
Respiration and airflow are used to look for periods of apnoea which occur when the patient stops breathing. These are then correlated with the sleep stage in which they occurred and the level the oxygen saturation fell to during the apnoea.