
 Computed tomography angiography (CTA) is a computed tomography technique used to visualize arterial and venous vessels throughout the body. This ranges from arteries serving the brain to those bringing blood to the lungs, kidneys, arms and legs.
Computed tomography angiography (CTA) is a computed tomography technique used to visualize arterial and venous vessels throughout the body. This ranges from arteries serving the brain to those bringing blood to the lungs, kidneys, arms and legs.
Technique
CT combines the use of x-rays with computerized analysis of the images. Beams of x-rays are passed from a rotating device through the area of interest in the patient's body from several different angles to obtain projection images, which then are assembled by computer into a three-dimensional picture of the area being studied.
A function for CTA is to Identify aneurysms in the aorta or in other major blood vessels. Aneurysms are diseased areas of a weakened blood vessel wall that bulges out-like a bulge in a tire. Aneurysms are life-threatening because they can rupture.
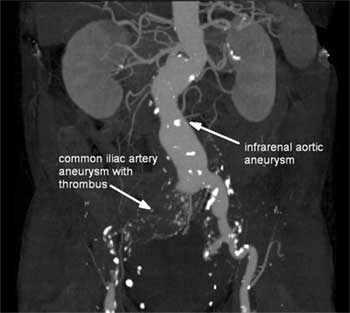 CTA for blood vessel examination. (Right.)
CTA for blood vessel examination. (Right.)
CTA can be used to examine blood vessels in many key areas of the body, including the brain, kidneys, pelvis, and the lungs. The procedure is able to detect narrowing of blood vessels in time for corrective therapy to be done.
This method displays the anatomical detail of blood vessels more precisely than magnetic resonance imaging (MRI) or ultrasound. Today, many patients can undergo CTA in place of a conventional catheter angiogram.
CTA is a useful way of screening for arterial disease because it is safer and much less time-consuming than catheter angiography and is a cost-effective procedure. There is also less discomfort because contrast material is injected into an arm vein rather than into a large artery in the groin.
Risks
There is a risk of an allergic reaction, which may be serious, whenever contrast material containing iodine is injected. A patient with a history of allergy to x-ray dye may be advised to take special medication for 24 hours before CTA to lessen the risk of allergic reaction or to undergo a different exam that does not call for contrast material injection. Compared with other imaging modalities, CTA is associated with a significant dose of ionizing radiation... Depending on patient age and exam protocol, CTA may cause a non-negligible increase in lifetime cancer risk. However, there are many clinical situations for which the benefits of performing the procedure outweigh this risk.
CTA for Endovascular aneurysm repair
 Endovascular aneurysm repair (EVAR) was first pioneered in the early 1990s. Since then technology of the devices has rapidly progressed and EVAR is now widely used as treatment of thoracic and abdominal aortic aneurysms.
Endovascular aneurysm repair (EVAR) was first pioneered in the early 1990s. Since then technology of the devices has rapidly progressed and EVAR is now widely used as treatment of thoracic and abdominal aortic aneurysms.
It is performed in patients undergoing elective aneurysm repair as well as patients undergoing emergency repair (eg. traumatic aortic injury and ruptured AAA).
Pros and cons
As with any new technique there are advantages and disadvantages to the traditional open repair. The advantages of endovascular repair are that they are less invasive than open surgery, have a lower surgical morbidity and mortality rate, and they reduce the length of post-operative stay in hospital. The disadvantages are likely to reduce over time. First of all is cost (stent-grafts and their delivery system are very expensive, plus the cost of any adjunctive procedures). Secondly the need for life-long follow-up imaging and the long-term durability of graft material is yet to be proven.
Technique
EVAR is performed by inserting a stent-graft into the lumen of the aneurysmal portion of the aorta. The stent-graft consists of a graft that provides a conduit for blood flow and a stent that anchors the graft to the aorta and provides structural support for the graft material. The aim is to divert blood flow into the graft, thereby bypassing the aneurysm.
Depending on the institution, EVAR is performed by interventional radiologists, vascular surgeons or both together. The patient typically requires a general anaesthetic. A stent-graft is inserted via the common femoral artery and deployed once it is confirmed in adequate position under the image intensifier, similar to other types of stent insertion. However, the diameter of the stent-graft and its delivery device are large (usual delivery device size ranges between 18 and 24 French), thus the procedure typically requires surgical exposure and closure of the common femoral artery, although percutaneous arterial access methods are also available.
Stent-grafts are made in a number of configurations. In AAA repair, the most common configuration is a bifurcated graft extending from the aorta into the common iliac or external iliac arteries. This typically requires access via both common femoral arteries. The grafts are modular in construction, that is, they are assembled in the patient in stages. The main body is deployed first, followed by the iliac limbs. The materials used in the stent-graft vary with each manufacturer but most grafts are made of expanded polytetrafluoroethylene (ePTFE) or woven polyester, and most stents are made of nitinol or stainless steel.
The key to successful EVAR is proper pre-procedural planning. Not all aneurysms are suitable for EVAR, depending on the anatomy of the aneurysm and iliac vessels. For those deemed suitable, careful aneurysm measurements are made with CTA that will ensure the graft is the correct length and diameter. If the graft is too short the aneurysm will not be excluded from the circulation; if it is too long important branch vessels may be inadvertently occluded; and if it is too narrow in diameter there will not be an adequate seal against the aortic wall which may result in an endoleak.
Adjunctive procedures
Adjunctive procedures are sometimes required to improve the technical success of EVAR just prior to or during endovascular repair. These include angioplasty of stenoses before device delivery, angioplasty of stenosis in the graft, embolisation of branch vessels to prevent endoleak, and stent reinforcement of endograft limb.
Complications
Recognised complications include:
- endoleak : occurs in ~ 30 to 40%
- continued enlargement of the aneurysm sac without endoleak
- delayed aneurysm rupture
- graft migration
- branch vessel occlusion with end-organ ischaemia / infarction
- infection
- stent-graft structural breakdown
- groin complications.
Patients require life-long imaging surveillance to monitor for endoleak, aneurysm expansion and graft integrity. This is most commonly performed via CTA. MRA is an alternative but stainless steel stents cause major susceptibility artefact that limits its usefulness in such cases. Different CT techniques have been advocated - single phase CTA, dual phase CTA (non contrast & arterial phase, or arterial and delayed phase), and triple phase CTA (non contrast, arterial phase and delayed phase). The need for non-contrast and delayed phase images is controversial, particularly in light of the cumulative radiation dose the patient will receive over the rest of their life. However, delayed imaging is felt to be important in order to detect slow endoleaks that do not show in the arterial phase.
Sources:
http://healthmetz.com/2011/06/17/signs-and-symptoms-of-abdominal-aortic-aneurysm.html
http://www.bupa.co.uk/individuals/health-information/directory/a/aortic-aneurysm#textBlock189238
http://en.wikipedia.org/wiki/Computed_tomography_angiography
http://radiopaedia.org/articles/endovascular-aneurysm-repair
http://www.imagingpathways.health.wa.gov.au/includes/dipmenu/aaa/image.html
Compiled and edited by John Sandham





