Action Learning as an accelerant for change
The NHS clinical leaders network states:
‘Action Learning is a method for individual and organisation development based on small groups of colleagues meeting over time to tackle real problems. Its roots are in adult learning and organisational development, ensuring that individuals can continue to be supported in their roles and learn from colleagues’.
(NHS Clinical Leaders Network, 2017)
I chose Action Learning as a targeted participative transformational tool for understanding transformative opportunities where the participants and I, as the researcher, interacted in the production of new knowledge, that is, improved technology and asset management system developed from the Action Learning cycle. Drawing on my previous research and studies, I developed a pedagogical process for Action Learning. I chose Action Learning because I needed an open methodology that allowed flexibility and openness when working with the participants.
As Carr and Kemmis note:
Action researchers accept that transformations of social reality cannot be achieved without engaging the understanding of the social actors involved.
(Carr & Kemmis, 2006, p. 181)
In Action Research (AR), social praxis is the point of departure or arrival in the construction or re-signification of knowledge. This allows the process of knowledge to be dynamically built in multiple layers with the NHS participants, working across many professional boundaries. The healthcare technology management study has been carried out in the participants’ natural environment under consideration, that is, the NHS Hospital. The flexibility of AR procedures is essential and the methodology allows for continual adjustments in accordance within the structure of the study. AR methods enable the continual transformational exercise of cyclic spirals such as: planning; action; reflection; research; review; transformation; and re-planning. This allows for actions that can be adjusted to meet the participant needs and participant/researcher reflections. The relevance of my healthcare experience and technology subject-knowledge allows me to use this developed ‘know-how’ to assist the participants in evaluating the study data that they themselves understand and put forward, bringing about practical knowledge of how to transform healthcare technology management, and knowledge, that can be improved and delivered in practice.
Pedagogical dynamics (‘learning by doing’) require that I ensure involvement, participation, commitment and production of new knowledge in collaboration with the participants at this NHS Hospital. The participants must be given priority in the AR process. The pedagogical AR processes that I feel are important to this case study are summarised as follows: Bringing together collective knowledge; re-signification of the cyclic spirals to re-assess current practice; production of new knowledge for the improvement of healthcare technology management; analysis/redirection and evaluation of practices; and awareness of the new dynamics of understanding.
It was necessary to establish methods for the question of how research and action come together in practice. The work highlights the fact that AR, structured according to its generating principles, is pedagogical research. This case study, being a transformational and pedagogical exercise, is configured as an action that tests healthcare practice, starting from ethical principles behind the continual formation and emancipation of the participants’ practice. From a methodological point of view the case study articulates the ontology of the participants and myself. The methodology is that of dialogical, participative and transforming principles and practices. Establishing the grounds for using AR (within a perspective of a scientific case study) at the Hospital requires that the transformation is imagined in an open manner, in which science is not synonymous with positivism, functionalism, and other labels.
My case study uses an AR approach and involves working closely with selected participants from the core professional practice areas most closely involved in healthcare technology management and practice. The intention of the project is to unfreeze opportunities, enabling transformational changes. Once the transformative changes have been agreed by the participants, executive approval (through a project board) is required to implement, then temporarily re-freeze for an agreed term, one year in this case. Re-freezing allows for further analysis to assess the success of the changes agreed. The Hospital has thus learnt from the project and has the opportunity to unfreeze and restart the planning process at agreed intervals, thus understanding that transformation is not a ‘once for all time’ exercise but rather, there will be an ongoing need to for managed cycles of ‘unfreezing’ and ‘refreezing’.
Action research cycles for Hospital healthcare technology transformation
An important point to make during this process was that all the participants were positive and interested in making a difference, because they all had responsibilities for specific areas of practice. The AR tool for healthcare technology transformation is outlined below in three steps:
1. INPUT (Preparatory)
2. ACTION (Informative)
3. OUTPUT (Transformational).
 To work, this AR tool requires an experienced researcher with detailed knowledge of the subject area (healthcare technology in this case) to take control of the case study thereby ‘unfreezing’ the current state. (Step 1)
To work, this AR tool requires an experienced researcher with detailed knowledge of the subject area (healthcare technology in this case) to take control of the case study thereby ‘unfreezing’ the current state. (Step 1)
I, as the researcher, used my work-based experience to assess the current state of healthcare technology management and any other available data that is coming from the Hospital or external agencies. Once the Hospital management had accepted that I would lead the case study process, the scope of the project needed to be agreed with them. When the scope was agreed, I was then able to use my specialist knowledge, working with the Hospital management team, to select the most appropriate participants who could collaborate and be able to influence other stakeholders in the Hospital. Once the participants were selected, they were approached to see if they had the time, and were willing and able to take part in the case study.
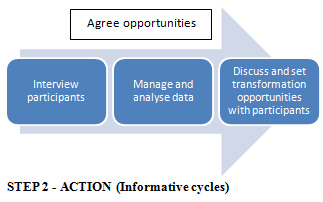 The participants were then signed up to being part of this transformational project (Step 2), they needed to be interviewed in a semi-structured way to ensure that their thoughts for improvement were confidentially recorded and documented. It was also important to follow up on a regular basis with each of the participants throughout the project, which meant regular planned meetings to discuss momentum and any potential changes in direction. The data being gathered at all times needed to be managed and analysed with the participants for further transformational opportunities. In this case study, the opportunities were discussed with the participants at a monthly meeting throughout the project. Separate meetings were held on a one-to-one basis with each of the participants, sometimes on a weekly basis to re-affirm commitment, discuss any new ideas, and give feedback from the project.
The participants were then signed up to being part of this transformational project (Step 2), they needed to be interviewed in a semi-structured way to ensure that their thoughts for improvement were confidentially recorded and documented. It was also important to follow up on a regular basis with each of the participants throughout the project, which meant regular planned meetings to discuss momentum and any potential changes in direction. The data being gathered at all times needed to be managed and analysed with the participants for further transformational opportunities. In this case study, the opportunities were discussed with the participants at a monthly meeting throughout the project. Separate meetings were held on a one-to-one basis with each of the participants, sometimes on a weekly basis to re-affirm commitment, discuss any new ideas, and give feedback from the project.
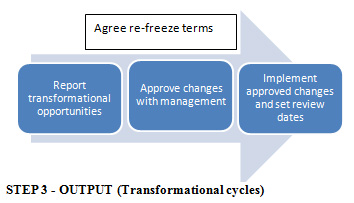 During the output cycle (Step 3), there was an objective to improve the medical devices management policy through collaboration with experience stakeholders. a one-to-one basis with each of the participants, sometimes on a weekly basis to re-affirm commitment, discuss any new ideas, and give feedback from the project.
During the output cycle (Step 3), there was an objective to improve the medical devices management policy through collaboration with experience stakeholders. a one-to-one basis with each of the participants, sometimes on a weekly basis to re-affirm commitment, discuss any new ideas, and give feedback from the project.
Some of the participants were executive level managers within the Hospital. The collaborative methods required reporting progress to the executive and allowing them to also participate in the process. The participants’ ideas for improvement were taken into account in all cycles but, ultimately, the output cycle would require sign off and agreement by the senior management committees. For this reason, it was important to have some of the senior managers acting as participants. That allowed their influence to be taken into consideration, and allowed them to be immersed in the transformation of policy, thus enabling them to convince their colleagues (who were not participants) to support the approval.

Conclusion
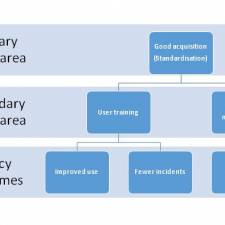
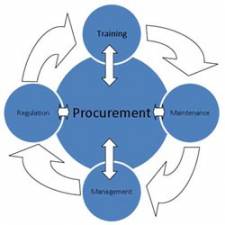
The current study is leading me to the conclusion that ‘Action Learning’ supported by ‘Action Research’ allows NHS Trusts to accelerate transformative change. In this ongoing study, we are concentrating on healthcare technology. AR is delivering a better understanding of how healthcare technology can be applied to deliver better healthcare in a sustainable and more affordable way, delivering better practice in areas such as procurement, training, maintenance, and management.
Bibliography
Carr, Wilfred and Kemmis, Stephen. 2006. Becoming Critical. Oxon : RouteledgeFalmer, 2006.
NHS Clinical Leaders Network. 2017. Action Learning. NHS Clinical Leaders Network. [Online] 2017. [Cited: April 28, 2017.]
http://www.cln.nhs.uk/aboutcln/action-learning.html.