
 In the past there was only one type of transthoracic defibrillation, that of a standard dampened sine wave monophasic shock.
In the past there was only one type of transthoracic defibrillation, that of a standard dampened sine wave monophasic shock.
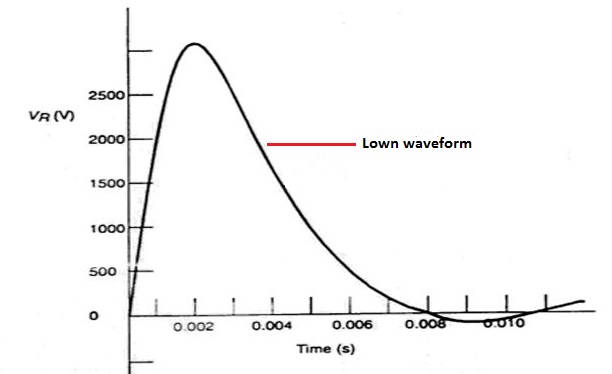
For decades, until the mid 90s, external defibrillators delivered a Lown type monophasic waveform, which was a heavily damped sinusoidal impulse having a mainly uniphasic characteristic.
Over many years of study, the theory of impedance and timing of shocks resulted in the standard monophasic practice of 25lbs of pressure (if using paddles) with three "stacked shocks". The key has been the sequential raising of the energy from 200j, to 300j, to a maximum of 360j, then having the subsequent shocks at 360j.
Monophasic versus biphasic waveforms.
With a monophasic waveforms, current flows in one direction, from one electrode to the other, stopping the heart so it has the chance to re-start on its own.
 Biphasic defibrillation alternates the direction of the pulses, completing one cycle in approximately 12 milliseconds. Biphasic defibrillation was originally developed and used for implantable cardioverter-defibrillators.
Biphasic defibrillation alternates the direction of the pulses, completing one cycle in approximately 12 milliseconds. Biphasic defibrillation was originally developed and used for implantable cardioverter-defibrillators.
With a biphasic waveform, current flows in one direction in phase 1 of the shock and then reverses for the phase 2. First used in commercially implantable defibrillators, biphasic waveforms are now the "gold standard" for these devices.
Research shows that biphasic waveforms are more effective and pose less risk of injury to the heart than monophasic waveforms, even when the shock energy level is the same. This is why manufacturers of external defibrillators are now using biphasic waveforms in their devices.
Although biphasic defibrillation is more effective than monophasic, the International guidelines published by the American Heart Association (AHA) state: Defibrillation Waveforms and Energy Levels 2010 (No Change From 2005): Data from both out-of-hospital and in-hospital studies indicate that biphasic waveform shocks at energy settings comparable to or lower than 200-J monophasic shocks have equivalent or higher success for termination of VF. However, the optimal energy for first-shock biphasic waveform defibrillation has not been determined. Likewise, no specific waveform characteristic (either monophasic or biphasic) is consistently associated with a greater incidence of ROSC or survival to hospital discharge after cardiac arrest. In the absence of biphasic defibrillators, monophasic defibrillators are acceptable. Biphasic waveform shock configurations differ among manufacturers, and none have been directly compared in humans with regard to their relative efficacy. Because of such differences in waveform configuration, providers should use the manufacturer’s recommended energy dose (eg, initial dose of 120 to 200 J) for its respective waveform.
Studies have shown that initially there is significant ST segment changes associated with high-energy defibrillation, which can last up to several months (if the patient survives).

The truncated exponential biphasic waveform, in which the polarity is reversed part way through the pulse, has been used in internal pacemakers for many years. There have been many studies done to prove some of the following points: With the Biphasic system there is higher success rate of initial shock conversion from VT (ventricular tachycardia) or VF (ventricular fibrillation) than monophasic (85.2% monophasic vs. 97.6% biphasic), The joules are significantly less (200j monophasic, 130 + 20j biphasic) which will affect reserve energy needs, Biphasic is more effective in reversing sustained VF.
Biphasic defibrillation therefore offers equal or better efficacy at lower energies than traditional monophasic waveform defibrillators-with less risk of post-shock complications such as myocardial dysfunction and skin burns. The underlying physiologic mechanisms aren't fully understood yet, but it's clear that biphasic waveforms lower the electrical threshold for successful defibrillation. Unlike monophasic devices, biphasic defibrillators use different waveform technologies: either a biphasic truncated exponential (BTE) wave or a rectilinear biphasic wave.
Types of waveforms

The biphasic truncated exponential waveform was originally developed for low-impedance internal cardiac defibrillation applications. It's been adapted for external defibrillation.
The second BTE defibrillator uses a high-energy (over 200 joules) protocol. This approach is promoted as easier to adopt but exposes patients to potentially higher peak currents.
 The rectilinear biphasic waveform was developed specifically for external defibrillation and takes into account high and varied patient impedance levels (the blocking of current flow caused by chest hair, large chest size, and poor electrode-to-chest contact). The rectilinear waveform maintains a stable shape in response to impedance, and the constant current in the first phase reduces potentially harmful peak currents.
The rectilinear biphasic waveform was developed specifically for external defibrillation and takes into account high and varied patient impedance levels (the blocking of current flow caused by chest hair, large chest size, and poor electrode-to-chest contact). The rectilinear waveform maintains a stable shape in response to impedance, and the constant current in the first phase reduces potentially harmful peak currents.
The BTE waveform was developed for internal use, where impedance is low. When it's used in a transthoracic device such as a defibrillator, impedance affects the waveform's shape. Research has shown that as the biphasic waveform's shape changes, its efficacy varies. The rectilinear waveform remains stable in shape, however, and current delivery dynamics are similar for patients over a wide range of impedances. This reduces the potentially adverse effect of patient impedance on successful defibrillation.
How do the different types of biphasic waveforms respond to patient impedance? When impedance is low (50 ohms), a 360-joule BTE defibrillator delivers more current than required, exposing the patient to potentially harmful high peak currents. At an average patient impedance of 75 ohms, the 360-joule BTE and 200-joule rectilinear defibrillators are equally effective. With high-impedance (greater than 100 ohms), the 200-joule rectilinear shock delivers a higher average current than a 360-joule BTE shock, therefore making it more effective at lower energy levels.
Higher energy doesn't necessarily mean you'll be raising the average current delivered. In a recently published study, researchers found that a high-energy BTE defibrillator needs nearly 50% more energy to deliver the same average current as a low-energy rectilinear defibrillator.
Five studies, with more than 900 human participants, have compared the efficacy of biphasic versus monophasic waveforms. These studies all used low-energy shocks (200 joules or less); no studies address the safety and efficacy of high-energy biphasic defibrillation (greater than 200 joules). The initial randomised human trial showed that a low-energy 130-joule BTE shock was clinically equal to a 200-joule monophasic shock. Low-energy shocks also were associated with substantially less post-shock ST-segment depression than high-energy monophasic shocks. Another study found that a 130-joule BTE shock was clinically equal to a 200-joule monophasic shock but that low-energy BTE shocks appeared to be less effective when transthoracic impedance was high.
An out-of-hospital study evaluated the efficacy of giving three shocks with a low-energy (150-joule) BTE defibrillator and found this combination 100% effective for converting VF. Patients defibrillated with low-energy biphasic shocks also had better neurological outcomes compared with those who had conventional high-energy shocks.
Rectilinear biphasic waveform. A study of 184 patients undergoing electro-physiology testing, ICD placement, or ICD testing found that first-shock efficacy for a 120-joule rectilinear waveform was statistically superior to a 200-joule monophasic waveform (99% versus 93%). For difficult-to-defibrillate patients (those with transthoracic impedance greater than 90 ohms), the 120-joule rectilinear shock was 100% effective on the first try, compared with 63% effectiveness for the 200-joule monophasic shock. Other studies have found that low-energy rectilinear shocks are more effective in converting atrial fibrillation than higher-energy monophasic shocks.
Without head-to-head comparisons of the two types of biphasic waveforms, it's too early to call either technology better or worse than the other. Both, however, are generally effective at lower energy levels when compared with monophasic defibrillation. Published peer-reviewed studies that have compared biphasic and monophasic technology generally show that BTE waveforms are equivalent to 200-joule monophasic waveforms and rectilinear shocks are superior.
 When applied to external defibrillators, biphasic defibrillation significantly decreases the energy level necessary for successful defibrillation, decreasing the risk of burns and myocardial damage.
When applied to external defibrillators, biphasic defibrillation significantly decreases the energy level necessary for successful defibrillation, decreasing the risk of burns and myocardial damage.
Ventricular fibrillation (VF) could be returned to normal sinus rhythm in 60% of cardiac arrest patients treated with a single shock from a monophasic defibrillator. Most biphasic defibrillators have a first shock success rate of greater than 90%.
When sudden cardiac arrest strikes, CPR alone doesn't save lives - it is merely a temporary measure that maintains minimal oxygen flow to the brain. Early defibrillation is required to re-establish a regular heartbeat.
A defibrillator can deliver a controlled electrical shock to a heart that has a life-threatening rhythm, such as ventricular fibrillation (VF). In VF, the heart's chaotic activity prevents blood from pumping to the body and brain.
Voltage stored by the defibrillator conducts electrical current (a shock) through the chest by way of electrodes or paddles placed on the chest. This brief pulse of current halts the chaotic activity of heart, giving the heart a chance to re-start with a normal rhythm.
The defibrillator uses energy to deliver a shock.
The amount of energy used depends on:
- How much voltage is used
- How much current is delivered
- The duration (length) of the shock
Energy is measured in joules (J). External defibrillators may offer a range of energy selections. So-called "low energy" defibrillators are those that limit their energy selections to 200J or less. Escalating energy defibrillators offer a range of energies, starting with low energy levels with the option to increase the energy levels for subsequent shocks.
Many people confuse current and energy. This distinction is important in defibrillation, since defibrillators are often described in terms of energy (e.g., 200J) but it is their current - not the energy - that defibrillates. Successful defibrillation requires that enough current be delivered to the heart muscle during the shock.
A wave of electrical current has a shape that can be drawn as a "waveform". The waveform shows how the flow of current changes over time during the defibrillation shock. The highest part of the current waveform is called "peak current". Too much peak current during the shock can injure the heart. It's the peak current (not energy) that can injure the heart.
Defibrillation requires a true middle-of-the-road approach. You must have enough current reach the heart to defibrillate the heart (stop the lethal rhythm), but not so much peak current that you risk damaging the heart. In fact, low-energy shocks from some defibrillators deliver higher peak current than higher-energy shocks from other types of defibrillators.
Impedance is the body's resistance to the flow of current. Some people naturally have higher impedance than others.
Certain factors can also increase impedance, such as:
- A large and/or hairy chest
- Very dry skin
- Excess air in the lungs
- Improper application of the defibrillation electrodes
You can't tell if someone has high impedance simply by looking at him or her. If impedance is high, the heart may not receive enough current for defibrillation to be successful. More current may be delivered by increasing the voltage and by increasing the energy selected (more joules) on the defibrillator.
Biphasic waveforms adjust for impedance by varying the characteristics of their waveforms. How each waveform adjusts for impedance has important consequences - it may determine whether or not someone's life is saved.
It is important to know how each biphasic waveform adjusts for impedance to ensure that high-impedance persons will have the same chance for survival as those who are easily defibrillated.
Many clinical studies demonstrating the success of low-energy biphasic waveforms were conducted in electro-physiology labs under ideal conditions. In real life, cardiac emergencies are much less predictable. Many factors affect the chance of defibrillation success: time elapsed before the first shock is given, placement of the electrode pads, the person's impedance level and certain health conditions. Therefore, it may take more current, a longer shock duration, and/or increased voltage to ensure success. Current flow changes with time during a defibrillation shock. When drawn on a graph, this is known as a waveform. Hearts respond differently to different waveforms, which is why the introduction of biphasic waveforms to external defibrillators can have a positive impact.
Statement on Biphasic Waveforms - Resuscitation Council (UK)
Although the very first commercial defibrillator used a biphasic waveform for the treatment of ventricular defibrillation, commercial external defibrillators in the western world adopted monophasic waveforms at least 30 years ago, and these have been used almost exclusively until recently. Thus, much of our clinical experience comes from the use of monophasic waveforms.
Conventional defibrillators produce monophasic shocks where the current flows in one direction. Biphasic waveform technology has developed from electrophysiological work on the design of implantable defibrillators. With biphasic shocks the direction of current flow is reversed at some point (usually near half way) during the discharge from the machine. External defibrillators that utilise biphasic waveforms are now available and licensed for clinical use. These devices have a number of advantages. Low energy biphasic shocks are as effective as higher energy monophasic shocks. This may result in less damage to the myocardium and a reduced frequency of post-shock contractility and arrhythmic problems. It allows smaller, lighter batteries to be used with a lengthening of the defibrillator battery life.
Published evidence indicates that biphasic waveform shocks of 200 J or less are safe and have equivalent or higher efficacy than damped sinusoidal waveform shocks of 200 J or 350 J.
At present, different manufacturers of defibrillators use different energy levels. The precise waveforms used in biphasic shocks vary considerably with different models. The energy levels used with successive shocks may stay constant or escalate depending on the machine. Some of these parameters are programmable, and may be pre-selected by the user. At present, there is inadequate comparative data to be able to decide which is the most effective energy level, shock sequence, or biphasic waveform. It is therefore impossible to make definite recommendations. The Council considers that all currently available biphasic defibrillators have energy levels that are acceptable.
Further information about the joint statement published in the Medicines and Healthcare products Regulatory Agency (MHRA) Devices Alert 2003/0012
Several studies in animals and humans have shown that defibrillators using biphasic waveforms are more effective for terminating ventricular fibrillation (VF) than those using monophasic waveforms. At least four different biphasic defibrillators are commonly available. The biphasic waveforms delivered by these devices each have different waveform characteristics and impedance compensation schemes and, most importantly, different recommended energy levels. The optimal biphasic waveform, energy level and shock sequence (escalating energy versus fixed dose) has not been determined.
Early clinical studies with two of the available biphasic devices demonstrated improved efficacy, using lower energy levels, in comparison with monophasic defibrillators for termination of VF and cardioversion of atrial fibrillation (AF). 1-3 One of these devices uses a biphasic truncated exponential waveform and delivers shocks with a fixed energy level of 150 J (Philips Heartstream, Seattle, WA, USA). The other uses a rectilinear biphasic waveform and, when treating VF, the manufacturer recommends shock delivery with escalating energy levels of 120 J, 150 J, and 200 J (Zoll Medical, Burlington, MA, USA).
The manufacturer of another biphasic defibrillator recommends escalating energy levels of 200 J, 300 J, and 360 J (200 J, 200 J, 360 J is acceptable in the UK) when treating VF (Medtronic Physio-Control, Redmond, WA, USA) and an automated external defibrillator (AED) from a fourth manufacturer utilises a low, high, high sequence of unspecified energy (Survivalink, Minneapolis, MN, USA). There is some evidence from animal studies that these higher biphasic energies may be more effective than lower energies if transthoracic impedance is high,4,5 but this requires confirmation in human clinical studies.
The intention of the joint statement published in the Medicines and Healthcare products Regulatory Agency (MHRA) Medical Devices Alert 2003/0012 was to alert defibrillator users to the possibility of confusion caused by the fact that some biphasic defibrillators are designed to deliver shocks with lower energies than monophasic devices.6 This has caused confusion to users of manual and semi-automatic defibrillators who are not fully familiar with the defibrillator available to them, particularly when they have wanted to deliver a 200J, 200J, 360J sequence but found that their particular biphasic defibrillator will deliver only lower energies. Those that may have to use defibrillators should use the energy levels indicated in the relevant manufacturer's instructions.
This potential for confusion is compounded because at present there is no "standard energy sequence" that can be applied to all defibrillators that use biphasic waveforms; the energy levels recommended by the various manufacturers are different. Therefore the 200 J, 200 J, 360 J sequence of shocks recommended by the European Resuscitation Council (ERC) and the Resuscitation Council (UK) for use with monophasic defibrillators is not appropriate as a generic approach for all biphasic devices.
This should not be interpreted to mean that it is inappropriate to use an escalating sequence of shocks of 200 J and above when this is recommended by a manufacturer of a specific biphasic defibrillator, provided that there is technical and clinical evidence to suggest that this is both safe and effective.
Until further data on the comparative efficacy of these biphasic devices become available, the Statement on Biphasic Waveforms made by the Resuscitation Council (UK) in September 2002 remains valid.
References:
Mittal S, Ayati S, Stein KM, Knight BP, Morady F, Schwartzman D, et al. Comparison of a novel rectilinear biphasic waveform with a damped sine wave monophasic waveform for transthoracic ventricular defibrillation. ZOLL Investigators. J Am Coll Cardiol 1999; 34: 1595-601.
Schneider T, Martens PR, Paschen H, Kuisma M, Wolcke B, Gliner BE, et al. Multicenter, randomized, controlled trial of 150-J biphasic shocks compared with 200- to 360-J monophasic shocks in the resuscitation of out-of-hospital cardiac arrest victims. Optimized Response to Cardiac Arrest (ORCA) Investigators. Circulation 2000; 102: 1780-7.
Mittal S, Ayati S, Stein KM, Schwartzman D, Cavlovich D, Tchou PJ, et al. Transthoracic cardioversion of atrial fibrillation: comparison of rectilinear biphasic versus damped sine wave monophasic shocks. Circulation 2000; 101: 1282-7.
Walker RG, Melnick SB, Chapman FW, Walcott GP, Schmitt PW, Ideker RE. Comparison of six clinically used external defibrillators in swine. Resuscitation 2003; 57: 73-83.
Niemann JT, Walker RG, Rosborough JP. Ischemically Induced Ventricular Fibrillation (VF): A Comparison of Fixed and Escalating Energy Defibrillation. Acad Emerg Med 2003; 10: 454.
Dr John Sandham
Sources:
https://www.ebme.co.uk/articles/clinical-engineering/49-internal-defibrillator-cardioverter
http://www.resus.org.uk
http://www.mhra.gov.uk
https://en.wikipedia.org/wiki/Defibrillation
http://www.heart.org/idc/groups/heart-public/%40wcm/%40ecc/documents/downloadable/ucm_317350.pdf



