The Lungs
The lungs consist of two cone shaped spongy organs that contain alveoli and trap air for gas exchange. The lung is designed for gas exchange. Its prime function is to allow oxygen to move from the air into the venous blood and carbon dioxide to move out. Although the lung performs other functions, its primary responsibility is to exchange gas. Oxygen and carbon dioxide (CO2) move between air and blood by simple diffusion that is from an area of high to low partial pressure. Ficks Law of diffusion states that the amount of gas that moves across a sheet of tissue is proportional to the area of the sheet but inversely proportional to its thickness.
The airways consist of a series of branching tubes which become narrower, shorter, and more numerous as they penetrate deeper into the lung. The trachea divides into right and left main bronchi, which in turn divide into lobar, then segmental bronchi. The process continues down to the terminal bronchioles, which are the smallest airways outside the alveoli. All these bronchi make u p the conducting airways. Their function is to lead inspired a ir to the gas exchanging regions of the lungs. Since conducting airways contain no alveoli, they do not participate in gas exchange. The terminal bronchioles divide into respiratory bronchioles, which have few alveoli. Finally, we come the alveolar ducts that are completely lined with alveoli. This alleviated area of the lung where gas exchange occurs is called the respiratory zone.
During inspiration, the volume of the thoracic cavity increases and air is drawn into the lung. The increase in volume is brought about partly by contraction of the diaphragm and partly by the actions of the intercostals muscles. These muscular actions increase the size of the thoracic cavity and air flows in due to the reduced pressure inside the chest (inhalation; governed by Boyles law which states that the pressure of a gas is inversely proportional to its volume). Inspired air flows down to the terminal bronchioles by bulk flow. Beyond that point, the combined cross-sectional area of the airways is so enormous because of the large number of branches, that the forward velocity of the gas becomes very small. Diffusion of gas within the airways then takes over as the dominant mechanism of ventilation in the respiratory zone. The rate of diffusion within the airways is so rapid, and the distances covered arson short, that differences in concentration within the alveoli are virtually abolished within a second.
An increase in thoracic volume results in a decrease in intrapulmonary pressure causing air to be pushed out of the lungs (exhalation). The lung is elastic and returns passively to its pre-aspiratory volume during resting breathing. It is remarkably easy to distend. For example, a normal breath of about 500 ml requires distending pressure of 3 cm water. By contrast, a balloon may need a pressure of up to 30 cm water f or the same change in volume.
Blood in need of oxygenation enters both lungs via the pulmonary arteries (from the hearts right ventricle). Oxygenated blood leaves the lungs through the pulmonary veins to the hearts left atrium. Air inspired through the nose, is passed through the trachea and bronchea, eventually entering the terminal bronchioles which supply the alveoli or air sacs, each 0.2mm in diameter. An estimated 300 million alveoli are contained in the lungs, generating up to 50 square metres of internal surface area at a lung volume of 3000ml.(The area of an average tennis court).
This gives rise to a total lung capacity of:
3.6 litres to 9.4 litres in an adult male.
2.5 litres to 6.9 litres in an adult female.
Respiration
Respiration is the interchange of gases between an organism and the medium in which it lives. Internal respiration is the exchange of gases between the blood stream and nearby cells.
The mechanics of respiration
Inspiration results from the contraction of the diaphragm and intercostal muscles. The rib cage swings upwards and outwards. The enlarged cavity housing the lungs undergoes a pressure reduction (-3 mm Hg) with respect to the pressure existing outside the body. Since the lungs are passive (no muscle tissue), they expand due to the positive external pressure.
e.g. if the environmental pressure is 760 mm Hg, the lung pressure is 757 mm Hg upon inspiration.
Expiration results from the relaxation of the diaphragm and intercostal muscles. The rib cage moves inward and downwards. The elastic recoil of the lungs creates a higher than atmospheric intrapulmonic pressure (plus 3 mm Hg) that forces air out of the lungs.
Parameters of respiration
Tidal Volume
The volume of gas inspired or expired during each respiratory cycle. Typically 500 ml.
Inspiratory reserve volume
The maximum amount of gas that can be inspired from the end-aspiratory position.
Expiratory reserve volume
Amount of air that can be forced out of lungs after normal expiration Typically 1200 ml
Residual volume
The volume of gas remaining in the lungs at the end of a maximum expiration. Typically 1200 ml.
Totaling capacity
The amount of gas contained in the lung at the end of a maximum inspiration.
Vital capacity
The maximum volume of gas that can be expelled from the lungs following a maximum inspiration.
Tidal volume, plus insp.reserve volume, plus exp.eserve volume. Typically 4800 ml.
Inspiratory capacity
The maximum volume of gas that can be inspired from the resting expiratory position. Typ.3600 ml.
Inspiritory reserve volume
Additional volume that can be inspired after a normal inspiration. Typically 3100 ml.
Functional residual capacity
The volume of gas remaining in the lungs at the resting end-expiratory position. Typically 2400 ml.
Minute volume
The total volume of air ventilated over a minute period. Should be qualified either inspiratory or expiratory.
Maximum voluntary ventilation
The maximum volume of air that can be ventilated per minute (also referred to a Maximum Breathing Capacity).
Total lung capacity
Amount of gas contained in lungs at end of maximum inspiration Typically 6000 ml.
Lung compliance
(The pulmonary volume change per unit pressure change).
Essentially, lung compliance is the ability of the alveoli and lung tissue to expand on inspiration. In clinical terms it is defined as the volume increase in the lungs per unit increase in the lung pressure. While clearly not a complete description of the pressure-volume properties of the lung, it is nevertheless useful in practice as a measure of the comparative stiffness of the lung. The stiffer the lung, the less the compliance. Compliance is reduced by diseases which cause an accumulation of fibrous tissue in the lung or by oedema in the alveolar spaces. It is increased in pulmonary emphysema and also with age, probably because of alterations in the elastic tissue in both cases.
There are two types of compliance, static and dynamic.
The static compliance of the lung is the change in volume for a given change in transpulmonary pressure with zero gas flow.
Dynamic compliance measurements are made by monitoring the tidal volume used, while intra thoracic pressure measurements are taken during the instance of zero air flow that occur at the end inspiritory and expiratory levels with each breath.
Lung compliance varies with the size of the lungs; a child has a smaller compliance than an adult does. Furthermore the volume-pressure curve is not linear, hence compliance does not remain constant. Fortunately, over the tidal volume range in which dynamic compliance measurements are usually performed, the relationship is approximately linear and a constant compliance is assumed. Compliance values are given as litres per cm of water.
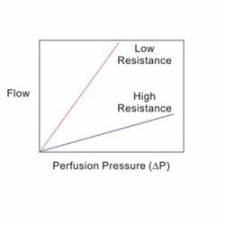
Airway resistance
Airway resistance relates to the ease with which air flows through tubular respiratory structures. Higher resistance occurs in smaller tubes such as bronchioles and alveoli that have not emptied properly. It is a pneumatic analogy of hydraulic or electrical resistance(R=V/I) and, as such, is a ratio of pressure to flow. Thus for the determination of airway resistance, intra alveolar pressure and airflow measurements are required. As was the case with compliance, airway resistance is not constant over the respiratory cycle. As pressure in the thoracic cavity becomes more negative, the airways are widened and the resistance is lowered. Conversely, during expiration, when the pressure in the thorax becomes positive, the airways are narrowed and resistance is increased. The intra alveolar pressure is given in cm water and the flow in litres per second; the airway resistance is expressed in cm water per litre per second.
Lung elasticity
Lung elasticity is the ability of the lung elastic tissues to recoil during expiration. The lungs should return to rest state easily to ensure sufficient exhaust of gas. Intra-thoracic pressure is the positive and negative pressure occurring within the thoracic cavity. These are critical to proper inspiration (negative internal pressure) and expiration (positive internal pressure). Intra alveolar pressure is of importance in maintaining proper respiration and gas exchange to and from the blood.
Only a portion of the air entering the respiratory system actually reaches the alveoli. The volume of air that is not available for gas exchange with the blood resides in the conducting spaces, known as 'dead air' and fills dead spaces consisting of and 150 ml.
Patient lung ventilators
Patients lung ventilators connect to the patients airway and are designed to replace or augment the patients ventilation automatically. They are used with a mask, endotracheal tube, (within the trachea) or tracheostomy tube (through an artificial opening in the trachea via the throat).
Most ventilators are positive pressure during inhalation to inflate the lungs with various gases or mixture of gases (air, oxygen, carbon dioxide, helium). Expiration is usually passive, although under certain conditions pressure may be applied during expiratory phase as well, in order to improve arterial oxygen tension. Only in rare circumstances is negative airway pressure utilised during expiration.
Most ventilators are operated in any of three modes
- Assistor mode.
- Controller mode.
- Assistor/controller mode.
These three modes differ only in the method by which inspiration is initiated.
Assistor mode: Inspiration is triggered by the patient. A pressure sensor responds to the slight negative pressure that occurs each time a patient attempts to inhale and triggers are equipment to begin inflating the lungs. Thus, the ventilator helps the patient inspire when he wants to breathe. A sensitivity adjustment is provided to select the amount of patient effort required to trigger the ventilator. The assistor mode is used for patients who are able to control the breathing but are unable to inhale a sufficient amount of air without assistance, or for whom the breathing requires too much effort (i.e. asthmatics, pulmonary pneumonia, etc.)
Controller mode: Breathing is controlled by a timer set to provide the desired respiration rate. Controlled ventilation is required for patients who are unable to breathe on their own. In this mode, the ventilator has complete control over the patients respiration and does not respond to any respiratory effort on the part of the patient.
Assistor/controller mode: The ventilator is normally triggered when the patient attempts to breathe (as in the assistor mode). However, if the patient fails to breathe within a pre-determined time, a timer automatically triggers the ventilator to inflate the lungs. Thus the patient controls his own breathing as long as he can, but if he should fail to do so, the equipment is able to take-over for him. On the other hand, this mode can be used to wean the patient from the controlled ventilation. If the patient attempts to breathe during controlled ventilation, the equipment will sense the attempt and operate in the assist mode immediately, irrespective of which part of the control phase it had reached.
Ventilators in clinical use can be classified into two main groups:
- Pressure cycled
- Volume cycled.
Pressure cycled, positive pressure, controller or assistor/controller type.
This device is powered pneumatically from a source of gas and requires no electrical power. The equipment in this category may contain an electrically powered compressor, or can be used with a separate compressor to commence ventilation with ambient air. Timing for operation in the controller mode is accomplished by filling a chamber with a gas and letting it bleed off through an adjustable needle valve. Pressure cycle ventilators can be quite small, but at the same time they can incorporate all the necessary equipment to control the flow of gas, mixed air and oxygen, sense the patients efforts to inspire, terminate inspiration when the desired pressure is reached, permit adjustment of the sensitivity of the triggering mechanism and the desired pressure level, and even generate negative pressure to assist expiration of some devices. In the assistor/controller type, a special type of valve senses the small negative pressure created by patients attempts to breathe.
Volume cycled ventilators use either a piston or bellows to dispense precisely controlled volume for each breath. In the intensive care setting where patients have pulmonary abnormalities and require calculated volumes (derived from blood gas analysis) and concentrations of gas, this type of ventilator is preferred. It is much larger than the pneumatically operated ventilator and electrically operated to provide a much greater degree of control over the ventilation than the pressure cycle types. Most volume-cycled equipments have adjustable pressure limits and alarms for safety. Also, their provision for adjusting pressure limits, and both inspiritory and expiratory times, can be used in conjunction with the volume setting to ensure therapeutic pulmonary function in the patient who needs it most. Volume cycle ventilators used in most intensive care units are always supplied with a spirometer to permit accurate monitoring of the patients ventilation.
Other available features may include a humidifier, and optional capabilities for negative pressure and positive end expiratory pressure (P. E. E. P.)
Non- invasive ventilation (CPAP/BiPAP)
Use of CPAP and BiPAP
There is evidence that CPAP (Continuous Positive Airway Pressure) and BiPAP (Bilevel Positive Airway Pressure) are effective in preventing need for intubation and also decreasing mortality in patients with Acute Respiratory Failure in properly selected patients.
Noninvasive treatment doesn't involve the use of surgery to provide breathing assistance; it relies on the use of masks and mouthpieces to deliver air.
BiPAP differs from CPAP in that the pressure during expiration may be adjusted separately from the pressure delivered during inspiration. This ability to set independent pressures during inhalation and exhalation result in lower average airway pressures than those produced by nasal CPAP.
Bi-PAP stands for Bilevel Positive Airway Pressure. The use of Bi-PAP machines is often called non-invasive face mask ventilation. This is because the trachea is not intubated so there is less trauma to the airway and more importantly there is a lower incidence of nosocomial infections.
CPAP delivers a continuous positive air pressure, most frequently at about 10 cm of water. This is delivered throughout the respiratory cycle and has been described as being similar to breathing with your head stuck out of a moving car. Continuous means that the pressure delivered to the patient is the same for any given breath. C-PAP can actually increase the work of breathing and be lethal to some patients.
BiPAP (Bilevel) means that the pressure varies during each breath cycle. When the user inhales, the pressure is similar to C-PAP. When they exhale, the pressure drops, making it much easier to breath. Inhale, pressure rises, exhale, pressure drops. BiPAP delivers CPAP but also senses when an inspiratory effort is being made and delivers a higher pressure during inspiration. When flow stops, the pressure returns to the CPAP level. This positive pressure wave during inspirations unloads the diaphragm decreasing the work of breathing. This form of ventilation has been used for years in patients with chronic respiratory failure due to neuromuscular problems or chest wall abnormalities. In patients with respiratory failure, a common technique is begin with the expiratory level at 5 and the inspiratory level at 15. The levels are adjusted based on patient comfort tidal volume achieved and blood gases.
As the use of BiPAP machines has increased, their cost has gone down. There are also more types of masks available and this has has improved patient comfort and compliance. The use of BiPAP machines is often called non-invasive face mask ventilation. This is because the trachea is not intubated so there is less trauma to the airway and more importantly there is a lower incidence of nosocomial infections.
Bi-PAP is a registered trademark of Respironics, Inc. Other manufacturers make VPAP and Bilevel machines that provide this same basic feature.
Sometimes you will see a "ST" behind Bi-PAP, VPAP, or Bilevel. The ST stands for Spontaneous Timed. This means that if the user does not breath on their own, the machine will initiate a breath for them. This feature is very useful in treating central sleep apnea and a host of pulmonary disorders.
For those patients who present to the emergency department with acute respiratory failure but with normal levels of consciousness, no major secretion problems and who are hemodynamically stable, a trial of BiPAP or CPAP could be attempted prior to considering intubation and a mechanical ventilator.
John Sandham IEng MIIE MIHEEM
Article updated 28/2/05
Article updated 31/12/10
References:
- depts.washington.edu/uwmedres/program/itc/ventilators.pdf
- n.b. link reported dead as of 31 Dec 10 - www.corexcel.com/courses/body_vent5.htm
- n.b. link reported dead as of 6 April 05 - http://www.books.md/L/dic/lungcompliance.php
- www.cyber-north.com/anatomy/respirat.htm
- n.b. link reported dead as of 6 April 05 - http://www.inforesp.org/about%20ventilation.htm
- http://www.guideline.gov/summary/summary.aspx?view_id=1&doc_id=3753
- http://www.focusonals.com/cpap_and_a_bipap.htm
- http://www.theberries.ns.ca/Archives/CPAP.html