100 years ago, medical equipment was in low demand and very low volumes. There were very few people buying equipment within the organisation, which made its procurement more easily managed. The purchasing of medical equipment had less impact and was therefore much less important than nursing and medical care. At that time, it was logical for Hospital managers to allow those people using medical devices have the authority, against an agreed budget, to choose and buy it.
Over the 100 following years, this authority has become part of the culture and also enshrined within Hospital budgets. This is now the normal way equipment is bought, and part of the structure within the finance and procurement mechanisms. This culture has not changed very much over the last 100 years, other than IT systems have been specifically designed around the procurement processes that relate to this culture. This has resulted in the organisations finance and procurement being based upon equipment choice and variety.
The diagram below is indicative of how the volume of devices has increased within a typical 800 bed hospital over time. This diagram represents the increasing use of technology that is typical across all hospitals. The volume of equipment being used in hospitals has increased tremendously over the last century. This growth is slowing down, but has not levelled out yet. The DTI has stated the Medical Technology market is estimated to continue growing at 10% per year for the next 5 years. (HM Government - Strength and opportunity, 2011)
 We need to question whether the foundations that the policy is built upon also need to be changed? There has been a significant growth in the numbers of equipment manufacturers designing and producing a wide range of choice and technology groups for nurses, doctors and other healthcare practitioners to use in the patient environment. Depending on the type of organisation, the number of different types of technology being used varies. Within an average 800 bed NHS Hospital trust, there are approximately 8000 devices in 400 technology groups that are used to deliver the patient services. Within these technology groups, there can be a wide variety of makes and models. It is possible to standardise to one device type from a single manufacturer for many device types.
We need to question whether the foundations that the policy is built upon also need to be changed? There has been a significant growth in the numbers of equipment manufacturers designing and producing a wide range of choice and technology groups for nurses, doctors and other healthcare practitioners to use in the patient environment. Depending on the type of organisation, the number of different types of technology being used varies. Within an average 800 bed NHS Hospital trust, there are approximately 8000 devices in 400 technology groups that are used to deliver the patient services. Within these technology groups, there can be a wide variety of makes and models. It is possible to standardise to one device type from a single manufacturer for many device types.
For example: A defibrillator can be reduced to a single type. It is therefore not necessary to have the level and variety of choice currently afforded to enable the delivery of safe cost effective services for the patient. We can improve on the current procurement policy with the prime objective being standardisation within technology groups, and increased utilisation within those technology groups. 
How does the equipment reach the patient?
Many equipment issues originate before the devices even arrives into our healthcare organisations. We must ask the question, 'How does the equipment get into our organisations?'
The diagram below shows there are many routes into the organisation: There are many routes for medical equipment to get into an organisation, including being bought from hospitals funds, donated by charity, rented, patient owned, loaned by a sales person, or brought in on an ambulance stretcher when a patient is transferred from another hospital.
There are many routes for medical equipment to get into an organisation, including being bought from hospitals funds, donated by charity, rented, patient owned, loaned by a sales person, or brought in on an ambulance stretcher when a patient is transferred from another hospital.
We especially need to look at the way equipment is bought from hospitals budgets and question why the budget holders at ward/department level have direct access to through their budgets to buy equipment. Why do these users (budget holders) continue to have such a variety of choice? This seems to be historic, and part of the culture within many healthcare organisations. Medical equipment users have been able to buy in this way for over 100 years.
This will has a severe impact on the amount of money being spent on medical devices, and the ease of delivery for user training and maintenance. One question that arises is, 'why do staff in the hospitals still have a high degree of choice when it comes to buying medical equipment?' This level of choice ultimately leads to higher costs and higher risks. Instead of trying to apply current best practice models, we must ask the question whether the current practice is right. Do procurement and finance systems need to be redesigned? If we started with a clean sheet? What could we achieve?
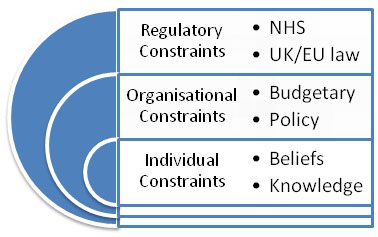
Current medical equipment policy and procurement models have been developed to meet the constraints of the regulators, the organisation, and the individual.
 These models can deliver improvements in terms of regulatory compliance and also cost savings. Although on the face of it, these models may be working somewhat effectively, when we drill more deeply into the underlying reasons that create risks and costs within a healthcare organisation, the same procurement culture still exists.
These models can deliver improvements in terms of regulatory compliance and also cost savings. Although on the face of it, these models may be working somewhat effectively, when we drill more deeply into the underlying reasons that create risks and costs within a healthcare organisation, the same procurement culture still exists.
Is there a possibility that we can create a new operational paradigm for equipment management policy?
The diagram below can at first seem very simple. Identify what you need, buy it, accept it into the organisation ensuring it meets specifications that were stated at the time it was bought, and then use it. This raises a number of questions, because when buying for a large organisation with thousands of pieces of equipment, it is important to understand how the business need is identified? As an individual, a consultant surgeon will definitely know what they want, and they will speak to their business manager telling them what to buy. Is this right? Should the consultant the deciding as an individual or should the organisation be speaking to all of the consultants in that field and making a decision that involves stakeholders, but allows standardisation within that technology group so that economic efficiency can be achieved, and training can be more easily achieved because there is less variety?
As an individual, a consultant surgeon will definitely know what they want, and they will speak to their business manager telling them what to buy. Is this right? Should the consultant the deciding as an individual or should the organisation be speaking to all of the consultants in that field and making a decision that involves stakeholders, but allows standardisation within that technology group so that economic efficiency can be achieved, and training can be more easily achieved because there is less variety?
Unfortunately, many consultants will put pressure on the management to have the devices they want. Their arguments can seem to make sense, and the managers are concerned that they may lose the services of that consultant. So, rather than upset the consultant, the business manager gets them the equipment that they prefer. Sometimes it is important to challenge these assumptions that consultants or any other practitioners using medical equipment should have their choice. A far better way would be to invite those consultants to be on a procurement committee that decides what is best for the organisation, the patient, and the equipment user.
Training is considered a high risk by the government, and as a result of this they have introduced the regulations previously discussed. The World Health Organisation recognises the benefits of medical equipment in their paper 'Increasing complexity of medical technology and consequences for training', but also point out the risks of underestimating the importance of training:
(World Health Organisation, 2010, p. 5)
To enable standardisation to happen requires changes to policy that ensures all purchasing of medical equipment is done in such a way as to include the users, but remove variety. The removal of the variety of devices within technology groups will lead to reduced costs, reduced risks, and easier training and maintenance.
When it comes to writing a medical devices management policy, we must work within the boundaries of the regulations and the organisational management structures. In our current good practice models, some organisations have already managed to reduce some of the variety of devices within technology groups. This has been achieved by setting up medical devices committees, and having all of the purchases approved through these committees.
The table below indicates the benefits of good procurement practice:
| Problems that effective procurement could avoid | Resulting waste you could save |
Policy/planning:
|
|
Procurement:
|
|
Training:
|
|
Operation and maintenance:
|
|
Although this has been partially successful in reducing the variety and cost, it still does not address the underlying ability of users to place orders for non-standard equipment, and therefore the current model only acts in a reactive way. In order to make a significant contribution to the understanding of the problem, we need to look more deeply at the regulatory constraints, the organisational constraints, and the individual constraints. What comes out of this debate is an understanding from those involved that even though we are doing better than in the past, we still have not properly addressed the problem which lies at the heart of this matter. That problem being, there is no planned procurement methodology for bringing devices into the organisation for the benefit of all stakeholders. (Patients, the organisation, and the users).
How do we overcome regulatory, organisational, and individual constraints that end up increasing risks to patients, and putting pressure on already tight budgets?
Poor procurement leads to variation and ultimately higher risks to the patient. This is recognised by research carried out by the World Health Organisation:
'New technologies are entering medical practice at an astounding pace. This is motivated in part by patients who request (and increasingly expect) minimally invasive procedures that result in minimal damage to healthy tissue. The 'side effects' resulting from the introduction of new, often-complex technology in health care, however, can be considerable-both for patients and health professionals. This paper has shown the consequences of the increased complexity of technology used for the treatment of patients.
Three facts emerged: 1) the devices are often not well designed for the medical environment in which they are used; 2) the user is often not trained properly to use these devices; and 3) the (new) procedures often result in long learning curves for health professionals.
These three facts influence outcome of care. It has been shown that it is valuable to develop a standardized methodology for the evaluation of the quality of medical devices and the analysis of complications resulting from their (mis)use. This can be done by introducing various methods, such as a video monitoring system. It is better that new equipment and instrumentation not be introduced without a thorough evaluation of its functionality (Technical Evaluation), followed by monitoring its use in clinical practice (Health Technology Assessment). These evaluations can be facilitated by a biomedical engineer or similar health-care professional. If the benefit of an instrument or device cannot be proven through these assessments, it should not be introduced. Standardization of equipment can solve many user problems; indeed this measure has been used effectively by aviation and industry. Training and (continuing) education are important components of standardization, to ensure safety. Any programmes standardizing medical practices and the use of medical devices could include training curricula, including credentialing methods for the post-training period (e.g. every half year). Implementing such measures as part of an overall programme of standardization will help to reduce errors and improve care.'
(World Health Organisation, 2010, p. 16)
The World Health Organisation has carried out a significant amount of research on medical devices management. Some areas of interest include:
- 65%of 145 countries have an authority responsible for implementing and enforcing medical device specific product regulations
- 34%of 145 countries have a health technology national policy that is part of the national health programme with only
- 9% of 145 countries having an independent health technology national policy
The UK does not have a national health technology policy. The current culture for equipment management and procurement is improving but still falls far behind many other countries. It is important to raise the profile of equipment management to ensure patients are kept safe and budgets are kept in the black.
Works Cited
HM Government - Strength and opportunity. (2011).
London: Department for Business, Innovation, and Skills. World Health Organisation. (2010, August).
Increasing complexity of medical technology and consequences for training and outcome of care. WHO.
Author: John Sandham IEng MIET MIHEEM Feb 2013